|
By Schon Roberts MD PGY-3 14 mo F, seen 3 days ago in ED with fever and possible UTI p/w new onset rash. She was placed on Omnicef and followed up with her regular doctor today. He sent her for evaluation. Parents state that she has had swelling of her hands and feet. Mother states that she has had a fever for 5 days. Fever was TMax 103 F. She has had adequate PO intake with good urine output and stooling. Parents deny URI Symptoms, N/V/D, or recent travel. Vital Signs show a pulse of 179, RR of 28, Temperature of 102.1 F, and patient has a spO2 of 99% on RA. Physical exam is remarkable for injected sclera, swelling of her hands and the dorsum of her feet. She has an erythematous rash on her trunk and extremities that blanches. It spares the palms and soles. Lungs are CTABL and cardiac exam is unremarkable. What is the best treatment option for this child? A. Broaden antibiotic coverage for meningitis to include listeria coverage, LP, and admit to the hospital B. Discharge home; Pt has a URI C. PO Tylenol, wait for defervescence, and D/C if improved D. Obtain an echocardiogram, start on high dose ASA, IVIG, and admit E. Start on steroids and admit with nephrology consult Answer D. Obtain an echocardiogram, start on ASA and IVIG, and admit Pathophysiology
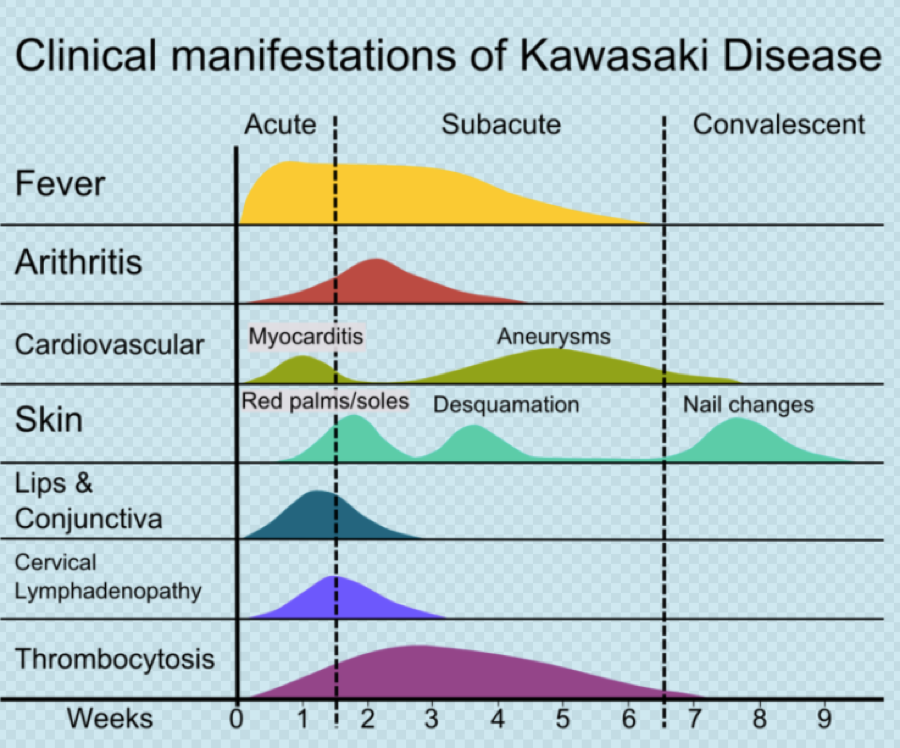
Symptoms/Exam Findings
 Labs
Diagnosis 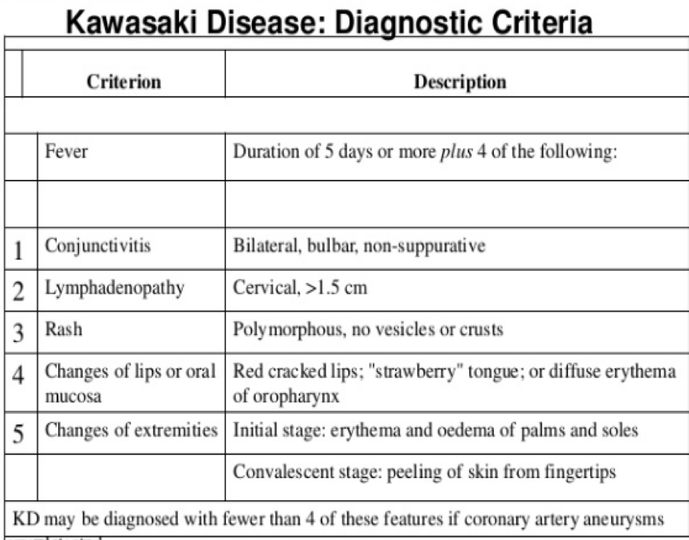  Incomplete Kawasaki Disease
Many patients present without all findings of Kawasaki Disease. To make the Dx: Three or more abnormal lab finding • Elevated CRP/ESR
Fever for >7 days w/o plausible different Dx Treatment
High vs. low dose IVIG Randomized multicenter Controlled Study showed:
Clinical Pearls
References 1."Newburger JW, Takahashi M, Gerber MA, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation 2004; 110:2747. 2. Furusho K, Kamiya T, Nakano H, et al. High-dose intravenous gammaglobulin for Kawasaki disease. Lancet 1984; 2:1055. 3.Newburger JW, Takahashi M, Burns JC, et al. The treatment of Kawasaki syndrome with intravenous gamma globulin. N Engl J Med 1986; 315:341. 4. Newburger JW, Takahashi M, Beiser AS, et al. A single intravenous infusion of gamma globulin as compared with four infusions in the treatment of acute Kawasaki syndrome. N Engl J Med 1991; 324:1633. 5. Durongpisitkul K, Gururaj VJ, Park JM, Martin CF. The prevention of coronary artery aneurysm in Kawasaki disease: a meta-analysis on the efficacy of aspirin and immunoglobulin treatment. Pediatrics 1995; 96:1057.
1 Comment
|
ABOUT USVegasFOAM is dedicated to sharing cutting edge learning with anyone, anywhere, anytime. We hope to inspire discussion, challenge dogma, and keep readers up to date on the latest in emergency medicine. This site is managed by the residents of Las Vegas’ Emergency Medicine Residency program and we are committed to promoting the FOAMed movement. Archives
June 2022
Categories |
 RSS Feed
RSS Feed
CONTACT US901 Rancho Lane, Ste 135 Las Vegas, NV 89106 P: (702) 383-7885 F: (702) 366-8545 |
ABOUT US |
WHO WE ARE |
WHAT WE DO |
STUDENTS |
RESEARCH |
FOAM BLOG |
© COPYRIGHT 2015. ALL RIGHTS RESERVED.
LasVegasEMR.com is neither owned nor operated by the Kirk Kerkorian School or Medicine at UNLV . It is financed and managed independently by a group of emergency physicians. This website is not supported financially, technically, or otherwise by UNLVSOM nor by any other governmental entity. The affiliation with Kirk Kekorian School of Medicine at UNLV logo does not imply endorsement or approval of the content contained on these pages.
Icons made by Pixel perfect from www.flaticon.com
Icons made by Pixel perfect from www.flaticon.com