|
By Emerson Posadas, MD, MBA (PGY-3) Thromboelastography (TEG) is a tool that measures in real-time clot development, stability, and dissolution. It not only measures the coagulation cascade, but also shows the interaction of platelets in clot formation. It is a dynamic measurement, that has in recent years, become more readily available in the emergency department. This blog will review the evidence behind its use in the Emergency Department in the setting of shock in both trauma and medical patients. First, we must review the basics of TEG and its interpretation. Keep in mind that TEG does not necessarily correlate with traditional coagulation measurements such as INR, PT/PTT, and total platelets. The general method of TEG involves measuring the physical properties of the clot by spinning whole blood in a cup with an electrical transducer. The strength of clot formation affects the rotation of the cup, which then generates data that is visualized in real time. There are several different tests available, some of which can measure fibrinogen and others that take into account whether the patient is on heparin. What may be difficult for many people first trying to interpret TEG results is that they are presented as not only values but also graphically. As emergency physicians, we have been trained to look at numbers and discrete ranges. Analyzing graphical data on the fly is a skillset many of us have not used in quite some time, if ever. What’s important to note, is that approximate normal ranges are also given; in the event one does not want to interpret the graphical data. Below is a very basic interpretation of the different values: 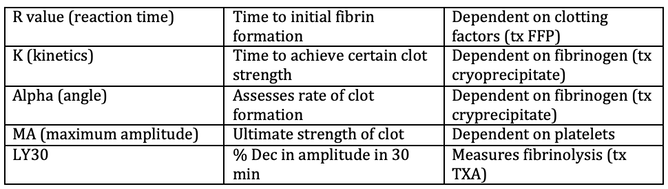 In broad terms, what are the indications for TEG? In general, TEG should not be ordered as a screening exam, but should only be used when a physician is considering an intervention, be it transfusing a patient or performing an invasive procedure. It can also be used to guide resuscitation, especially in the massive transfusion setting.1
The utility of TEG in guiding massive transfusions protocols, especially in the setting of trauma, is well studied.2 Since the PROPPR trial in 2015, 1:1:1 of FFTP:PLT:PRBC has been a mainstay for trauma resuscitation as it showed that more patients achieved hemostasis and fewer deaths due to exsanguination at 24 hours.3 However, transfusions of any type of blood product do pose serious risks. TEG-directed resuscitation has been explored as a tool that allows physicians to target specific coagulation parameters, with the idea that often less is more. In 2016, a randomized control trial compared TEG-directed resuscitation versus conventional coagulation assays in the trauma setting. In this study, with a sample size of 111, they found that TEG-guided massive transfusion protocols improved survival compared to those guided by conventional coagulation assays. TEG-directed resuscitation also resulted in less blood products being used.4 However, it is important to note prior to this study the recommendation from a Cochrane systemic review in 2015 stated that there was no evidence on the accuracy of TEG for trauma induced coagulopathy, and strongly suggest that at present these tests should only be used for research.5 Further complicating the issue, studies have since been published either in favor or against TEG-guided management. While controversy still exists in the trauma setting, there is even less clear evidence for the use of TEG-directed resuscitation in medical coagulopathies. There is some evidence for its use in post-partum hemorrhage, bleeding cirrhotic patients, GI bleeds, and severe epistaxis. However, currently many published articles regarding its use outside of the trauma setting are for very specific patient populations and/or case reports. In a recent randomized control trial, TEG-guided blood resuscitation was compared with conventional coagulation assays for patients with cirrhosis with nonvariceal bleeding. The study showed a significantly lower use of blood components in the TEG-guided resuscitation with similar mortality between the two groups.6 Within OBGYN, TEG has been studied for its use in guiding management of severe postpartum hemorrhage.7 The use of TEG to identify coagulation abnormalities in adult patients with sepsis has also been studied, but its exact applications have yet to be established. 8More studies need to be conducted to better understand the efficacy for its use in the emergency department. In summary, TEG-directed resuscitation has been more established in the trauma setting but remains controversial. Studies have only recently started regarding its use in the bleeding medical patient, many of which are not conducted in the emergency department setting. Regardless, TEG-directed therapy seems promising and should at least be considered by emergency department physicians for any patient with serious bleeding that may require transfusion.
2 Comments
|
ABOUT USVegasFOAM is dedicated to sharing cutting edge learning with anyone, anywhere, anytime. We hope to inspire discussion, challenge dogma, and keep readers up to date on the latest in emergency medicine. This site is managed by the residents of Las Vegas’ Emergency Medicine Residency program and we are committed to promoting the FOAMed movement. Archives
June 2022
Categories |
 RSS Feed
RSS Feed
CONTACT US901 Rancho Lane, Ste 135 Las Vegas, NV 89106 P: (702) 383-7885 F: (702) 366-8545 |
ABOUT US |
WHO WE ARE |
WHAT WE DO |
STUDENTS |
RESEARCH |
FOAM BLOG |
© COPYRIGHT 2015. ALL RIGHTS RESERVED.
LasVegasEMR.com is neither owned nor operated by the Kirk Kerkorian School or Medicine at UNLV . It is financed and managed independently by a group of emergency physicians. This website is not supported financially, technically, or otherwise by UNLVSOM nor by any other governmental entity. The affiliation with Kirk Kekorian School of Medicine at UNLV logo does not imply endorsement or approval of the content contained on these pages.
Icons made by Pixel perfect from www.flaticon.com
Icons made by Pixel perfect from www.flaticon.com